
Page 40 - Dental Practice August 2022
P. 40
40-41-Melissa article-Q8:18-22-Lanka Mahesh.qxd 8/17/2022 6:34 PM Page 1
restorative dentistry section
MITIGATING SECONDARY CARIES
MELISSA JOHNSON
INTRODUCTION
G.V. Black’s class I caries pathology is classified as simple (1 surface)
lesions that affect either the occlusal, buccal, or lingual aspects of
teeth. With only a single surface involved, the clinician may dispense
with the additional armamentarium needed to treat compound
(2 surfaces) or even complex (3 surface) caries. With the advent of
direct, adhesively-bonded composite resin, contemporary dentists
are able to deliver both minimally invasive and aesthetic results to
patients when restoring class I decay. Various intrinsic and extrinsic
factors including preparation designs, extension of pathologicala-
gents, patient’s overall caries risk, and the clinician’s ability to con-
trol moisture all add to the complexity and long-term success of
these otherwise straight forward composite restorations.
This case report begins with an evaluation of a re-care patient: a
healthy twenty six-year-old male presented for his routine cleaning
and exam. The exam revealed occlusal caries on six of his eight
molars, making him a high caries risk patient. Estimated sizes of the
lesions, age, salivary flow, oral hygiene and the use of a high strength
fluoride treatment were weighed and used as discussion points to
assist the patient and clinician in deciding on the best treatment out- FIG 1
comes. After reviewing all parameters, it was decided that conserva-
tive composite restorations would be in the patient’s best interest.
With no pain or sensitivity being reported by the patient, the
rational starting point was to treat the deepest decay first, teeth
numbers 18, 19 (international system: 36, 37). Teeth numbers 18
and 19 were pulp tested and responded normally to percussion and
cold testing. In an effort to mitigate risk factors and create a sound,
pain free restoration the following steps were taken:
Rubber Dam isolation to combat intraoral humidity and the
pooling of saliva at the back of the mouth, biomimetic technique-
sused in an effort to reduce stresses created by the high configura-
tion factor of the preparation, and finally, a high-quality polishing
technique to ensure minimal plaque retention and reduce risk of FIG 2 FIG 3 FIG 4
recurrent decay at the enamel composite margins.
dried.
PROCEDURE 6. Two layers of a universal adhesive [Zipbond, SDI Limited] were
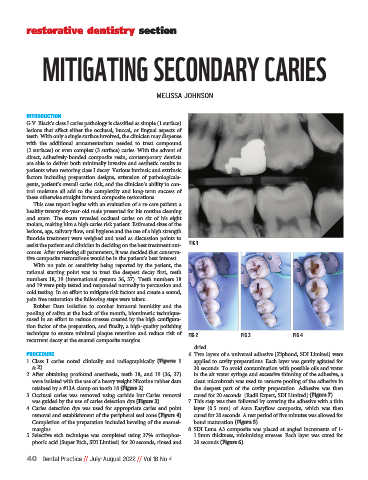
1. Class I caries noted clinically and radiographically (Figures 1 applied to cavity preparations. Each layer was gently agitated for
& 2). 30 seconds. To avoid contamination with possible oils and water
2. After obtaining profound anesthesia, teeth 18, and 19 (36, 37) in the air water syringe and excessive thinning of the adhesive, a
were isolated with the use of a heavy weight Nicotine rubber dam clean microbrush was used to remove pooling of the adhesive in
retained by a #13A clamp on tooth 18 (Figure 2). the deepest part of the cavity preparation. Adhesive was then
3. Occlusal caries was removed using carbide bur.Caries removal cured for 20 seconds. [Radii Expert, SDI Limited] (Figure 7).
was guided by the use of caries detection dye (Figure 3). 7. This step was then followed by covering the adhesive with a thin
4. Caries detection dye was used for appropriate caries end point layer (0.5 mm) of Aura Easyflow composite, which was then
removal and establishment of the peripheral seal zone (Figure 4) cured for 20 seconds. A rest period of five minutes was allowed for
Completion of the preparation included beveling of the enamel- bond maturation (Figure 5).
margins. 8. SDI Luna A3 composite was placed at angled increments of 1-
5. Selective etch technique was completed using 37% orthophos- 1.5mm thickness, minimizing stresses. Each layer was cured for
phoric acid [Super Etch, SDI Limited] for 20 seconds, rinsed and 20 seconds (Figure 6).
40 Dental Practice // July-August 2022 // Vol 18 No 4