
Page 48 - DP Vol 21 No1_Neat
P. 48
MULTIDISCIPLINARY
RETRACTION AND RESTORATION OF
ERRATIC IMPACTED CENTRAL INCISOR IN
CLOSE PROXIMATION OF AN ODONTOME:
A CLINICAL CASE REPORT
Gaurav Gupta, D.K Gupta, Neelja Gupta
INTRODUCTION
A person’s appearance is significantly influenced by the appearance of
their maxillary incisors when they speak and smile. Missing incisors
can also lead to functional issues, particularly when speaking or
producing sounds like “s.” Therefore, the proper eruption, position,
and morphology of these teeth are essential for both phonetics and
aesthetics.
The failure of maxillary incisor eruption typically becomes evident
during the mixed dentition period, usually between seven and nine
years of age. The maxillary incisor is the third most commonly
impacted tooth, with an incidence ranging from 0.06% to 0.2% .
1
Failure of eruption can be caused by various factors including
pathological defects, tooth deformities, ectopic positioning of the
tooth germ, pulpitis, ankylosed primary teeth, endocrine disorders, Fig 1a
or bony abnormalities. Obstructions may also include thick soft
tissue barriers due to early extractions, odontomas, cysts, or
supernumerary teeth. Trauma in the anterior region can result in
premature loss of deciduous teeth, dilaceration of the incisor, delayed
root development, or luxation. Changes in tooth morphology or
position may further hinder eruption, with the severity of damage
depending on the developmental stage of the tooth and the direction
of trauma .
2
Early orthodontic and surgical interventions are recommended
to prevent further deterioration of dental alignment. Impacted teeth
can be exposed using various surgical techniques prior to initiating
orthodontic correction. This article describes the management of a
case involving an erratic central incisor impaction in a patient with a
history of trauma 10 years back.
Fig 1b
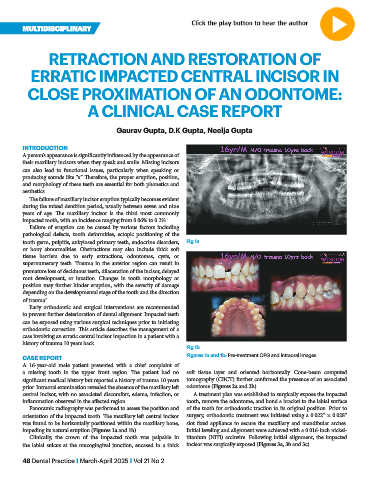
CASE REPORT Figures 1a and 1b: Pre-treatment OPG and intraoral images.
A 16-year-old male patient presented with a chief complaint of
a missing tooth in the upper front region. The patient had no soft tissue layer and oriented horizontally. Cone-beam computed
significant medical history but reported a history of trauma 10 years tomography (CBCT) further confirmed the presence of an associated
prior. Intraoral examination revealed the absence of the maxillary left odontome (Figures 2a and 2b).
central incisor, with no associated discomfort, edema, infection, or A treatment plan was established to surgically expose the impacted
inflammation observed in the affected region. tooth, remove the odontome, and bond a bracket to the labial surface
Panoramic radiography was performed to assess the position and of the tooth for orthodontic traction to its original position. Prior to
orientation of the impacted tooth. The maxillary left central incisor surgery, orthodontic treatment was initiated using a 0.022” × 0.028”
was found to be horizontally positioned within the maxillary bone, slot fixed appliance to secure the maxillary and mandibular arches.
impeding its natural eruption (Figures 1a and 1b). Initial leveling and alignment were achieved with a 0.016-inch nickel-
Clinically, the crown of the impacted tooth was palpable in titanium (NiTi) archwire. Following initial alignment, the impacted
the labial sulcus at the mucogingival junction, encased in a thick incisor was surgically exposed (Figures 3a, 3b and 3c).
48 Dental Practice I March-April 2025 I Vol 21 No 2