
Page 12 - DP20-2.qxd
P. 12
implantology section
PARTLY REMOVABLE CERAMIC
VENEERED BRIDGE ON IMPLANTS
A COMFORTABLE CONSTRUCTION
Tobias Rotter
Meeting the patient’s aesthetic requirements often presents a great
challenge when it comes to implant restorations. However, the most
crucial part is the selection of suitable materials. Overloading of the
ceramic due to a lack of the touch sensibility with fixed or partly
removable ceramic-veneered implant-supported constructions can
cause chipping or even fractures in the structure. In the following
article, the author describes in detail how to successfully produce a full
restoration consisting of partly removable ceramic-veneered bridges
on twelve implants.
The patient presented herself at my brother’s clinic and requested a
ceramic fixed implant-supported restoration. We, therefore, considered
an occlusal screw-retained construction with either a metal or metal-
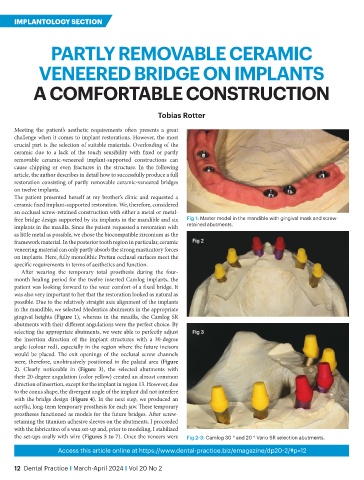
free bridge design supported by six implants in the mandible and six Fig 1: Master model in the mandible with gingival mask and screw-
implants in the maxilla. Since the patient requested a restoration with retained abutments.
as little metal as possible, we chose the biocompatible zirconium as the
framework material. In the posterior tooth region in particular, ceramic Fig 2
veneering material can only partly absorb the strong masticatory forces
on implants. Here, fully monolithic Prettau occlusal surfaces meet the
specific requirements in terms of aesthetics and function.
After wearing the temporary total prosthesis during the four-
month healing period for the twelve inserted Camlog implants, the
patient was looking forward to the wear comfort of a fixed bridge. It
was also very important to her that the restoration looked as natural as
possible. Due to the relatively straight axis alignment of the implants
in the mandible, we selected Medentica abutments in the appropriate
gingival heights (Figure 1), whereas in the maxilla, the Camlog SR
abutments with their different angulations were the perfect choice. By
selecting the appropriate abutments, we were able to perfectly adjust Fig 3
the insertion direction of the implant structures with a 30-degree
angle (colour red), especially in the region where the future incisors
would be placed. The exit openings of the occlusal screw channels
were, therefore, unobtrusively positioned in the palatal area (Figure
2). Clearly noticeable in (Figure 3), the selected abutments with
their 20-degree angulation (color yellow) created an almost common
direction of insertion, except for the implant in region 13. However, due
to the conus shape, the divergent angle of the implant did not interfere
with the bridge design (Figure 4). In the next step, we produced an
acrylic, long-term temporary prosthesis for each jaw. These temporary
prostheses functioned as models for the future bridges. After screw-
retaining the titanium adhesive sleeves on the abutments, I proceeded
with the fabrication of a wax set-up and, prior to modeling, I stabilized
the set-ups orally with wire (Figures 5 to 7). Once the veneers were Fig 2-3: Camlog 30 ° and 20 ° Vario SR selection abutments.
Access this article online at https://www.dental-practice.biz/emagazine/dp20-2/#p=12
12 Dental Practice I March-April 2024 I Vol 20 No 2