
Page 12 - DP Vol 21 No1_Neat
P. 12
ORAL SURGERY
PARTIAL EXTRACTION THERAPY:
THE ULTIMATE TISSUE PRESERVATION
TECHNIQUE
Ali Tunkiwala
In implant dentistry, it is well established that preserving the
labial bone post-extraction with conventional techniques is a
significant challenge. This difficulty arises because the labial bone
is embryologically derived from the tooth itself. Consequently,
a complete tooth extraction inevitably leads to the loss of the
labial plate. Given its inherent thinness, even the most atraumatic
extraction techniques can cause microcracks in this bone, leading
to its resorption. Clinically, this translates to mucosal recession and,
ultimately, esthetic failure.
Over the years, various strategies—including socket preservation,
immediate implant placement, and early implant placement—have
been explored to mitigate this loss. However, none have consistently
countered the consequences of buccal bone resorption. This is where
“Partial Extraction Therapy (PET)” has demonstrated remarkable
success. By employing the socket shield technique, PET capitalizes on
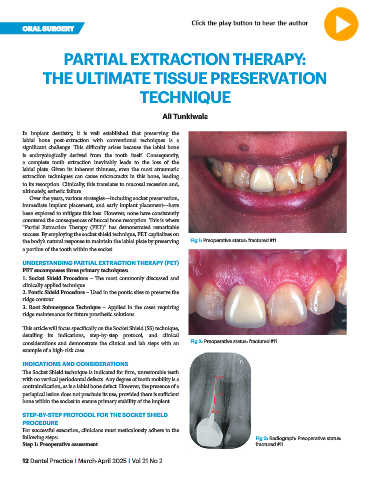
the body’s natural response to maintain the labial plate by preserving Fig 1: Preoperative status: fractured #11
a portion of the tooth within the socket.
UNDERSTANDING PARTIAL EXTRACTION THERAPY (PET)
PET encompasses three primary techniques:
1. Socket Shield Procedure – The most commonly discussed and
clinically applied technique.
2. Pontic Shield Procedure – Used in the pontic sites to preserve the
ridge contour.
3. Root Submergence Technique – Applied in the cases requiring
ridge maintenance for future prosthetic solutions.
This article will focus specifically on the Socket Shield (SS) technique,
detailing its indications, step-by-step protocol, and clinical
considerations and demonstrate the clinical and lab steps with an Fig 2: Preoperative status: fractured #11
example of a high-risk case.
INDICATIONS AND CONSIDERATIONS
The Socket Shield technique is indicated for firm, unrestorable teeth
with no vertical periodontal defects. Any degree of tooth mobility is a
contraindication, as is a labial bone defect. However, the presence of a
periapical lesion does not preclude its use, provided there is sufficient
bone within the socket to ensure primary stability of the implant.
STEP-BY-STEP PROTOCOL FOR THE SOCKET SHIELD
PROCEDURE
For successful execution, clinicians must meticulously adhere to the
following steps: Fig 3: Radiograph: Preoperative status:
Step 1: Preoperative assessment fractured #11
12 Dental Practice I March-April 2025 I Vol 21 No 2