
Page 20 - DP Vol 20 No 4 HR
P. 20
IMPLANT DENTISTRY SECTION
COMPLEX FULL MOUTH RESTORATION USING
IMPLANTS AND NATURAL TEETH -
A CASE OF FULL MOUTH REHABILITATION
D. Satyanarayana, Pavan Kishore, Mohit Suryavanshi
INTRODUCTION
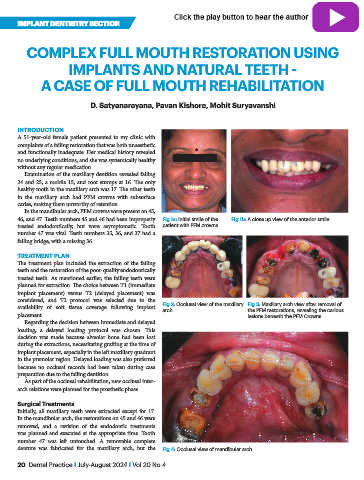
A 51-year-old female patient presented to my clinic with
complaints of a failing restoration that was both unaesthetic
and functionally inadequate. Her medical history revealed
no underlying conditions, and she was systemically healthy
without any regular medication.
Examination of the maxillary dentition revealed failing
24 and 25, a mobile 15, and root stumps at 16. The only
healthy tooth in the maxillary arch was 17. The other teeth
in the maxillary arch had PFM crowns with subsurface
caries, making them unworthy of retention.
In the mandibular arch, PFM crowns were present on 45,
46, and 47. Teeth numbers 45 and 46 had been improperly Fig 1a: Initial smile of the Fig 1b: A close up view of the anterior smile
treated endodontically, but were asymptomatic. Tooth patient with PFM crowns
number 47 was vital. Teeth numbers 35, 36, and 37 had a
failing bridge, with a missing 36.
TREATMENT PLAN
The treatment plan included the extraction of the failing
teeth and the restoration of the poor-quality endodontically
treated teeth. As mentioned earlier, the failing teeth were
planned for extraction. The choice between T1 (immediate
implant placement) versus T2 (delayed placement) was
considered, and T2 protocol was selected due to the Fig 2: Occlusal view of the maxillary Fig 3: Maxillary arch view after removal of
availability of soft tissue coverage following implant arch the PFM restorations, revealing the carious
placement. lesions beneath the PFM Crowns
Regarding the decision between immediate and delayed
loading, a delayed loading protocol was chosen. This
decision was made because alveolar bone had been lost
during the extractions, necessitating grafting at the time of
implant placement, especially in the left maxillary quadrant
in the premolar region. Delayed loading was also preferred
because no occlusal records had been taken during case
preparation due to the failing dentition.
As part of the occlusal rehabilitation, new occlusal inter-
arch relations were planned for the prosthetic phase.
Surgical Treatments
Initially, all maxillary teeth were extracted except for 17.
In the mandibular arch, the restorations on 45 and 46 were
removed, and a revision of the endodontic treatments
was planned and executed at the appropriate time. Tooth
number 47 was left untouched. A removable complete
denture was fabricated for the maxillary arch, but the Fig 4: Occlusal view of mandibular arch
20 Dental Practice I July-August 2024 I Vol 20 No 4