
Page 12 - DP Vol 22 No 1
P. 12
AESTHETICS
FULL MOUTH REHABILITATION OF AN ADULT WITH
ANTERIOR OPEN BITE AND DENTAL FLUOROSIS:
A TIME-CONSTRAINED, MINIMALLY INVASIVE,
DIGITALLY DRIVEN RESTORATIVE APPROACH
Harleen Gandhi, Ronil Kakodkar
INTRODUCTION
Anterior open bite in adults is traditionally addressed through orthodontic
therapy combined with orthognathic surgery, especially when skeletal
discrepancies are present. While this approach remains the gold standard
in many cases, it is not always feasible due to patient preferences, time
constraints, or previous unsuccessful orthodontic attempts.
With advancements in adhesive dentistry and digital planning,
restorative solutions can be considered in carefully selected patients. When
vertical dimension is stable, posterior support is intact, and neuromuscular
adaptation is favourable, a restorative full-mouth rehabilitation may offer
a predictable, conservative alternative.
This article presents the comprehensive adhesive rehabilitation of an
adult patient with anterior open bite and generalized dental fluorosis,
completed within a limited treatment window using a minimally invasive,
digitally guided workflow.
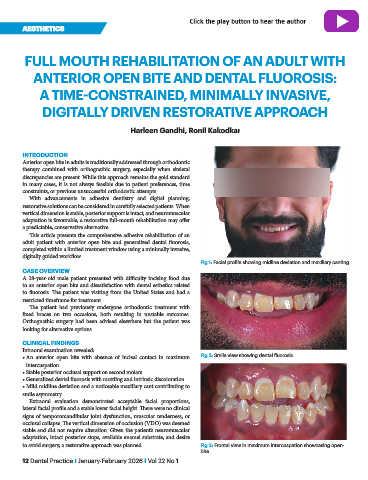
Fig 1: Facial profile showing midline deviation and maxillary canting
CASE OVERVIEW
A 28-year-old male patient presented with difficulty incising food due
to an anterior open bite and dissatisfaction with dental esthetics related
to fluorosis. The patient was visiting from the United States and had a
restricted timeframe for treatment.
The patient had previously undergone orthodontic treatment with
fixed braces on two occasions, both resulting in unstable outcomes.
Orthognathic surgery had been advised elsewhere but the patient was
looking for alternative options.
CLINICAL FINDINGS
Intraoral examination revealed:
• An anterior open bite with absence of incisal contact in maximum Fig 2: Smile view showing dental fluorosis
intercuspation
• Stable posterior occlusal support on second molars
• Generalized dental fluorosis with mottling and intrinsic discoloration
• Mild midline deviation and a noticeable maxillary cant contributing to
smile asymmetry
Extraoral evaluation demonstrated acceptable facial proportions,
lateral facial profile and a stable lower facial height. There were no clinical
signs of temporomandibular joint dysfunction, muscular tenderness, or
occlusal collapse. The vertical dimension of occlusion (VDO) was deemed
stable and did not require alteration. Given the patient’s neuromuscular
adaptation, intact posterior stops, available enamel substrate, and desire
to avoid surgery, a restorative approach was planned. Fig 3: Frontal view in maximum intercuspation showcasing open-
bite
12 Dental Practice I January-February 2026 I Vol 22 No 1