
Page 14 - DT14-1
P. 14
14-20-Mohit-Q8_6-7-8-Ivoclar.qxd 4/15/2024 8:01 PM Page 1
14 prosthetic section DENTAL TECHNOLOGY, JANUARY-MARCH 2024
A MINIMALLY INVASIVE APPROACH IN
REHABILITATION OF SEVERE EROSION WITH
COMPOSITE AND LITHIUM DI-SILICATE MATERIAL
PAVAN KISHORE NALLAPATI AND MOHIT SURYAVANSHI
CASE PRESENTATION
A 36-year-old female patient presented to our clinic with complaints of
tooth sensitivity and difficulty in chewing, accompanied by concerns
regarding low self-esteem due to a compromised smile and impaired chew-
ing function.
On clinical examination, we observed that there were generalised ero-
sive lesions on all the teeth except the upper anteriors and first premolars,
which were protected by zirconia crowns (Figure 2). There was a loss of
vertical dimension due to erosion and improper guidance during function-
al movements, leading to an impaired bite as described by the patient.
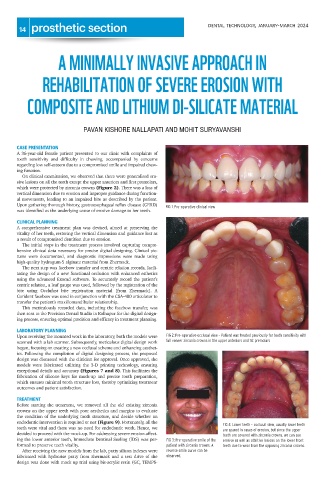
Upon gathering thorough history, gastroesophageal reflux disease (GERD) FIG 1: Pre-operative clinical view
was identified as the underlying cause of erosive damage to her teeth.
CLINICAL PLANNING
A comprehensive treatment plan was devised, aimed at preserving the
vitality of her teeth, restoring the vertical dimension and guidance lost as
a result of compromised dentition due to erosion.
The initial steps in the treatment process involved capturing compre-
hensive clinical data necessary for precise digital designing. Clinical pic-
tures were documented, and diagnostic impressions were made using
high-quality hydrogum-5 alginate material from Zhermack.
The next step was facebow transfer and centric relation records, facili-
tating the design of a new functional occlusion with enhanced esthetics
using the advanced Exocad software. To accurately record the patient’s
centric relation, a leaf gauge was used, followed by the registration of the
bite using Occlufast bite registration material [from Zhermack]. A
Corident facebow was used in conjunction with the CSA-400 articulator to
transfer the patient’s maxillomandibular relationship.
This meticulously recorded data, including the facebow transfer, was
then sent to the Precision Dental Studio in Kolhapur for the digital design-
ing process, ensuring optimal precision and efficacy in treatment planning.
LABORATORY PLANNING
Upon receiving the mounted work in the laboratory, both the models were FIG 2: Pre-operative occlusal view – Patient was treated previously for teeth sensitivity with
full veneer zirconia crowns in the upper anteriors and 1st premolars
scanned with a lab scanner. Subsequently, meticulous digital design work
began, focusing on creating a new occlusal scheme and enhancing aesthet-
ics. Following the completion of digital designing process, the proposed
design was discussed with the clinician for approval. Once approved, the
models were fabricated utilizing the 3-D printing technology, ensuring
exceptional details and accuracy (Figures 7 and 8). This facilitates the
fabrication of silicone keys for mock-up and precise tooth preparation,
which ensures minimal tooth structure loss, thereby optimizing treatment
outcomes and patient satisfaction.
TREATMENT
Before starting the treatment, we removed all the old existing zirconia
crowns on the upper teeth with poor aesthetics and margins to evaluate
the condition of the underlying tooth structure, and decide whether an
endodontic intervention is required or not (Figure 9). Fortunately, all the
FIG 4: Lower teeth - occlusal view, usually lower teeth
teeth were vital and there was no need for endodontic work. Hence, we are spared in cases of erosion, but since the upper
decided to proceed with the mock-up. For addressing severe erosion affect- teeth are covered with zirconia crowns, we can see
ing the lower anterior teeth, Immediate Dentinal Sealing (IDS) was per- FIG 3: Pre-operative smile of the erosive as well as attritive lesions on the lower front
formed to preserve teeth vitality. patient with zirconia crowns. A teeth due to wear from the opposing zirconia crowns.
After receiving the new models from the lab, putty silicon indexes were reverse smile curve can be
fabricated with hydrorise putty from zhermack and a test drive of the observed.
design was done with mock up trial using bis-acrylic resin (GC, TEMPS-