
Page 27 - DT 15-1
P. 27
26-29-Prandtner_6-7-8-Ivoclar.qxd 01-05-2025 07:45 Page 2
DENTAL TECHNOLOGY, JANUARY-MARCH 2025
implantology section 27
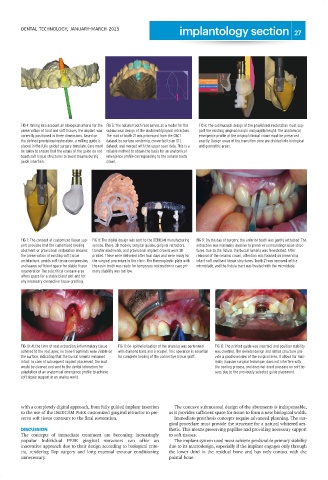
FIG 4: Taking into account all biological criteria for the FIG 5: The natural tooth root serves as a model for the FIG 6: The submucosal design of the provisional restoration must sup-
preservation of hard and soft tissues, the implant was submucosal design of the abutment/gingival retractors. port the existing gingival margin and papilla height. The anatomical
correctly positioned in three dimensions. Based on The root of tooth 21 was processed from the CBCT emergence profile of the original clinical crown must be preserved
the defined provisional restoration, a milling guide is dataset by surface rendering, converted to an STL exactly. Design areas of the transition zone are divided into biological
placed in the fully guided surgery template. Care must dataset, and merged with the upper scan data. This is a and geometric areas.
be taken to ensure that the edges of the guide do not reliable method to obtain the basis for an anatomical
touch soft tissue structures to avoid trauma during emergence profile corresponding to the natural tooth
guide insertion. crown.
FIG 7: The concept of customized tissue sup- FIG 8: The digital design was sent to the DEDICAM manufacturing FIG 9: On the day of surgery, the anterior tooth was gently extracted. The
port provides that the customized healing service. There, 3D models, surgical guides, gingival retractors, extraction was minimally invasive to preserve surrounding tissue struc-
abutment or provisional restoration ensures transfer abutments, and provisional implant crowns were 3D tures. Due to the fistula, the buccal lamella was fenestrated. After
the preservation of existing soft tissue printed. These were delivered after four days and were ready for removal of the ceramic crown, attention was focused on preserving
architecture, avoids soft tissue compression, the surgical procedure in the clinic. The thermoplastic plate with intact soft and hard tissue structures. Tooth 21 was removed with a
and leaves sufficient space for stable tissue the resin tooth was ready for temporary restoration in case pri- microblade, and the fistula tract was treated with the microblade.
regeneration The subcritical concave area mary stability was too low.
offers space for a stable blood clot and for
any necessary connective tissue grafting.
FIG 10: At the time of root extraction, inflammatory tissue FIG 11: De-epithelialization of the alveolus was performed FIG 12: The printed guide was inserted, and position stability
adhered to the root apex; no bone fragments were visible on with diamond balls and a scalpel. This operation is essential was checked. The skeletal design and lattice structure pro-
the surface, indicating that the buccal lamella remained for complete healing of the connective tissue graft. vide a good overview of the surgical area. It allows for mini-
intact. In case of subsequent implant placement, the root mally invasive surgical technique, does not interfere with
would be cleaned and sent to the dental laboratory for the cooling process, and does not exert pressure on soft tis-
adaptation of an anatomical emergence profile to achieve sues due to the previously selected guide placement.
soft tissue support in an analog world.
with a completely digital approach, from fully guided implant insertion The concave submucosal design of the abutments is indispensable,
to the use of the DEDICAM PEEK customized gingival retractor to pre- as it provides sufficient space for tissue to form a new biological width.
serve soft tissue contours to the final restoration. Immediate prosthesis concepts require advanced planning. The sur-
gical procedure must provide the structure for a natural whitered aes-
DISCUSSION thetic. This means preserving papillae and providing necessary support
The concepts of immediate treatment are becoming increasingly to soft tissues.
popular Individual PEEK gingival retractors can offer an The implant system used must achieve predictable primary stability
innovative approach due to their design according to biological crite- due to its macrodesign, especially if the implant engages only through
ria, rendering flap surgery and long mucosal contour conditioning the lower third in the residual bone and has only contact with the
unnecessary. palatal bone.