
Page 10 - DT Vol 15 No 3
P. 10
10 I implantology DENTAL TECHNOLOGY, JULY-SEPTEMBER 2025
FULL MOUTH REHABILITATION:
THE NEWER ALTERNATIVE FOR DENTURES
KOMAL RAJPUROHIT AND NIKHIL JADHAV
INTRODUCTION
Full-arch implant-supported rehabilitation has attracted considerable interest
in the recent years because it restores oral function and improves the quality
of life of the patients suffering from severe tooth loss. Oral rehabilitation for a
patient with severe bone and soft tissue loss presents a challenge to clinicians.
Here, we present the clinical case of a patient undergoing full-mouth
reconstruction with implant-supported fixed prostheses. We demonstrated
immediacy with implant placement and prosthesis. We believe that primary
stability during implant placement may have contributed to our success.
Dental implants and their prostheses are among the most researched
treatment options for partial or complete loss of teeth nowadays [1,2] . The
success rates of dental implants are directly influenced by preoperative
planning of implants in an optimal 3D position [3,4] .
Here, we present a case report of a patient suffering from generalized
chronic periodontitis. He underwent a full-mouth reconstruction with
dental implants. We successfully restored his oral function and esthetics with
fixed screw-retained implant-supported prostheses.
Fig 1
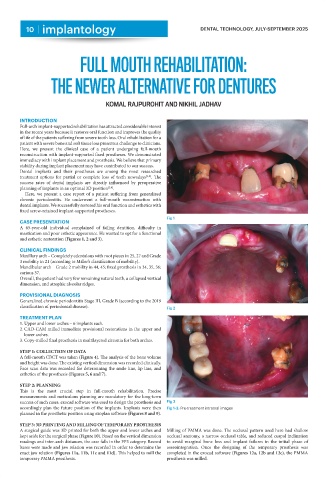
CASE PRESENTATION
A 65-year-old individual complained of failing dentition, difficulty in
mastication and poor esthetic appearance. He wanted to opt for a functional
and esthetic restoration (Figures 1, 2 and 3).
CLINICAL FINDINGS
Maxillary arch – Completely edentulous with root pieces in 25, 27 and Grade
3 mobility in 21 (according to Miller’s classification of mobility).
Mandibular arch – Grade 2 mobility in 44, 45; fixed prosthesis in 34, 35, 36;
carious 37.
Overall, the patient had very few remaining natural teeth, a collapsed vertical
dimension, and atrophic alveolar ridges.
PROVISIONAL DIAGNOSIS
Generalized chronic periodontitis Stage III, Grade B (according to the 2019
classification of periodontal disease). Fig 2
TREATMENT PLAN
1. Upper and lower arches – 6 implants each.
2. CAD-CAM milled immediate provisional restorations in the upper and
lower arches.
3. Copy-milled final prosthesis in multilayered zirconia for both arches.
STEP 1: COLLECTION OF DATA
A full-mouth CBCT was taken (Figure 4). The analysis of the bone volume
and height was done. The existing vertical dimension was recorded clinically.
Face scan data was recorded for determining the smile line, lip line, and
esthetics of the prosthesis (Figures 5, 6 and 7).
STEP 2: PLANNING
This is the most crucial step in full-mouth rehabilitation. Precise
measurements and meticulous planning are mandatory for the long-term
success of such cases. exocad software was used to design the prosthesis and Fig 3
accordingly plan the future position of the implants. Implants were then Fig 1-3: Pre-treatment intraoral images
planned in the prosthetic position using exoplan software (Figures 8 and 9).
STEP 3: 3D PRINTING AND MILLING OF TEMPORARY PROSTHESIS
A surgical guide was 3D printed for both the upper and lower arches and Milling of PMMA was done. The occlusal pattern used here had shallow
kept aside for the surgical phase (Figure 10). Based on the vertical dimension occlusal anatomy, a narrow occlusal table, and reduced cuspal inclination
readings and inter-arch distances, the case falls in the FP3 category. Record to avoid marginal bone loss and implant failures in the initial phase of
bases were made and jaw relation was recorded in order to determine the osseointegration. Once the designing of the temporary prosthesis was
exact jaw relation (Figures 11a, 11b, 11c and 11d). This helped to mill the completed in the exocad software (Figures 12a, 12b and 12c), the PMMA
temporary PMMA prosthesis. prosthesis was milled.