
Page 13 - DT Vol 15 No 3
P. 13
implantology I
DENTAL TECHNOLOGY, JULY-SEPTEMBER 2025 13
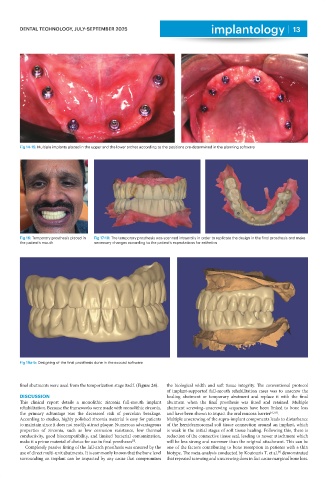
Fig 14-15: Multiple implants placed in the upper and the lower arches according to the positions pre-determined in the planning software
Fig 16: Temporary prosthesis placed in Fig 17-18: The temporary prosthesis was scanned intraorally in order to replicate the design in the final prosthesis and make
the patient’s mouth necessary changes according to the patient’s expectations for esthetics
Fig 19a-b: Designing of the final prosthesis done in the exocad software
final abutments were used from the temporization stage itself. (Figure 24). the biological width and soft tissue integrity. The conventional protocol
of implant-supported full-mouth rehabilitation cases was to unscrew the
DISCUSSION healing abutment or temporary abutment and replace it with the final
This clinical report details a monolithic zirconia full-mouth implant abutment when the final prosthesis was fitted and retained. Multiple
rehabilitation. Because the frameworks were made with monolithic zirconia, abutment screwing–unscrewing sequences have been linked to bone loss
the primary advantage was the decreased risk of porcelain breakage. and have been shown to impact the oral mucosa barrier [6,7,8] .
According to studies, highly polished zirconia material is easy for patients Multiple unscrewing of the supra-implant components leads to disturbance
to maintain since it does not readily attract plaque. Numerous advantageous of the hemidesmosomal soft tissue connection around an implant, which
properties of zirconia, such as low corrosion resistance, low thermal is weak in the initial stages of soft tissue healing. Following this, there is
conductivity, good biocompatibility, and limited bacterial contamination, reduction of the connective tissue seal, leading to newer attachment which
[5]
make it a prime material of choice for use in final prostheses . will be less strong and narrower than the original attachment. This can be
Completely passive fitting of the full-arch prosthesis was ensured by the one of the factors contributing to bone resorption in patients with a thin
use of direct multi-unit abutments. It is commonly known that the bone level biotype. The meta-analysis conducted by Koutouzis T. et al. demonstrated
[9]
surrounding an implant can be impacted by any cause that compromises that repeated screwing and unscrewing does in fact cause marginal bone loss.