
Page 27 - DP Vol 20 No 4 HR
P. 27
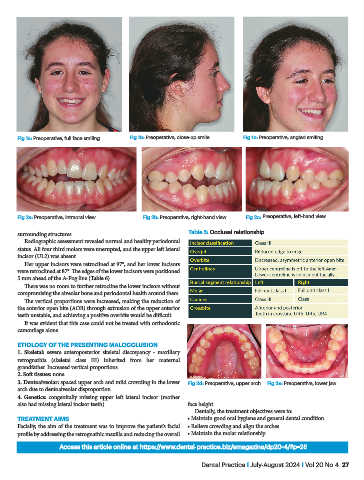
Fig 1a: Preoperative, full face smiling Fig 1b: Preoperative, close-up smile Fig 1c: Preoperative, angled smiling
Fig 2a: Preoperative, intraoral view Fig 2b: Preoperative, right-hand view Fig 2c: Preoperative, left-hand view
surrounding structures. Table 5: Occlusal relationship
Radiographic assessment revealed normal and healthy periodontal
status. All four third molars were unerupted, and the upper left lateral
incisor (UL2) was absent.
Her upper incisors were retroclined at 97°, and her lower incisors
were retroclined at 87°. The edges of the lower incisors were positioned
5 mm ahead of the A-Pog line (Table 6).
There was no room to further retrocline the lower incisors without
compromising the alveolar bone and periodontal health around them.
The vertical proportions were increased, making the reduction of
the anterior open bite (AOB) through extrusion of the upper anterior
teeth unstable, and achieving a positive overbite would be difficult.
It was evident that this case could not be treated with orthodontic
camouflage alone.
ETIOLOGY OF THE PRESENTING MALOCCLUSION
1. Skeletal: severe anteroposterior skeletal discrepancy - maxillary
retrognathia (skeletal class III) inherited from her maternal
grandfather. Increased vertical proportions
2. Soft tissues: none
3. Dentoalveolar: spaced upper arch and mild crowding in the lower Fig 2d: Preoperative, upper arch Fig 2e: Preoperative, lower jaw
arch due to dentoalveolar disproportion
4. Genetics: congenitally missing upper left lateral incisor (mother
also had missing lateral incisor teeth). face height.
Dentally, the treatment objectives were to:
TREATMENT AIMS • Maintain good oral hygiene and general dental condition
Facially, the aim of the treatment was to improve the patient’s facial • Relieve crowding and align the arches
profile by addressing the retrognathic maxilla and reducing the overall • Maintain the molar relationship
Access this article online at https://www.dental-practice.biz/emagazine/dp20-4/#p=26
Dental Practice I July-August 2024 I Vol 20 No 4 27