
Page 32 - DP Vol 20 No 4 HR
P. 32
IMPLANT DENTISTRY SECTION
IMMEDIATE LOADING AND FULL MOUTH
REHABILITATION WITH A 4 YEAR FOLLOW UP:
A CASE REPORT
Komal Rajpurohit and Nikhil Jadhav
INTRODUCTION
One well-researched treatment for partial or complete adontia is
dental implants [1,2] . Preoperative planning of the prosthesis has
a direct impact on the high success rates of dental implants [3,4] .
Contemporary CAD/CAM technology allows for the most precise
selection of dental implant size and location, as well as precise
implantation in accordance with preoperative planning. Nonetheless,
there is an ongoing debate on whether to use screw or cement
retained prosthetic constructions [5-8] . Achieving passive fit is one
of the main issues with a full-arch implant-supported prosthesis.
Assuming that the implant and framework surfaces are made exactly
plain, passivity is attained when both the antagonist surfaces, i.e., the
intaglio surface of the framework and the multi-units of the implants,
are in maximal congruency, with no stresses in the components after
the final tightening of the screws . The passive fit of the construction
[9]
may not be adequately secured by screw retention at the bone level
platform. Furthermore, problems with this kind of fixation might
range from implant fracture or failure of osseointegration to fracture
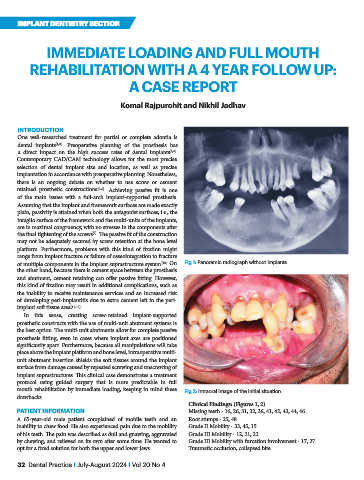
of multiple components in the implant suprastructure system . On Fig 1: Panoramic radiograph without implants
[10]
the other hand, because there is cement space between the prosthesis
and abutment, cement retaining can offer passive fitting. However,
this kind of fixation may result in additional complications, such as
the inability to receive maintenance services and an increased risk
of developing peri-implantitis due to extra cement left in the peri-
implant soft tissue area [11-13] .
In this sense, creating screw-retained implant-supported
prosthetic constructs with the use of multi-unit abutment systems is
the best option. The multi-unit abutments allow for complete passive
prosthesis fitting, even in cases where implant axes are positioned
significantly apart. Furthermore, because all manipulations will take
place above the implant platform and bone level, intraoperative multi-
unit abutment insertion shields the soft tissues around the implant
surface from damage caused by repeated screwing and unscrewing of
implant suprastructures. This clinical case demonstrates a treatment
protocol using guided surgery that is more predictable in full
mouth rehabilitation by immediate loading, keeping in mind these Fig 2: Intraoral image of the initial situation
drawbacks.
Clinical Findings: (Figures 1, 2)
PATIENT INFORMATION Missing teeth - 16, 26, 31, 32, 36, 41, 42, 43, 44, 46
A 65-year-old male patient complained of mobile teeth and an Root stumps - 25, 48
inability to chew food. He also experienced pain due to the mobility Grade II Mobility - 33, 45, 15
of his teeth. The pain was described as dull and gnawing, aggravated Grade III Mobility - 12, 21, 22
by chewing, and relieved on its own after some time. He wanted to Grade III Mobility with furcation involvement - 17, 27
opt for a fixed solution for both the upper and lower jaws. Traumatic occlusion, collapsed bite
32 Dental Practice I July-August 2024 I Vol 20 No 4