
Page 39 - DP Vol 21 No1_Neat
P. 39
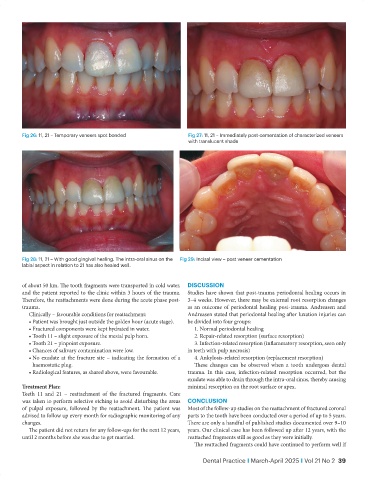
Fig 26: 11, 21 – Temporary veneers spot bonded Fig 27: 11, 21 – Immediately post-cementation of characterized veneers
with translucent shade
Fig 28: 11, 21 – With good gingival healing. The intra-oral sinus on the Fig 29: Incisal view – post veneer cementation
labial aspect in relation to 21 has also healed well.
of about 50 km. The tooth fragments were transported in cold water, DISCUSSION
and the patient reported to the clinic within 3 hours of the trauma. Studies have shown that post-trauma periodontal healing occurs in
Therefore, the reattachments were done during the acute phase post- 3–4 weeks. However, there may be external root resorption changes
trauma. as an outcome of periodontal healing post-trauma. Andreasen and
Clinically – favourable conditions for reattachment: Andreasen stated that periodontal healing after luxation injuries can
• Patient was brought just outside the golden hour (acute stage). be divided into four groups:
• Fractured components were kept hydrated in water. 1. Normal periodontal healing
• Tooth 11 – slight exposure of the mesial pulp horn. 2. Repair-related resorption (surface resorption)
• Tooth 21 – pinpoint exposure. 3. Infection-related resorption (inflammatory resorption, seen only
• Chances of salivary contamination were low. in teeth with pulp necrosis)
• No exudate at the fracture site – indicating the formation of a 4. Ankylosis-related resorption (replacement resorption)
haemostatic plug. These changes can be observed when a tooth undergoes dental
• Radiological features, as shared above, were favourable. trauma. In this case, infection-related resorption occurred, but the
exudate was able to drain through the intra-oral sinus, thereby causing
Treatment Plan: minimal resorption on the root surface or apex.
Teeth 11 and 21 – reattachment of the fractured fragments. Care
was taken to perform selective etching to avoid disturbing the areas CONCLUSION
of pulpal exposure, followed by the reattachment. The patient was Most of the follow-up studies on the reattachment of fractured coronal
advised to follow up every month for radiographic monitoring of any parts to the tooth have been conducted over a period of up to 5 years.
changes. There are only a handful of published studies documented over 9–10
The patient did not return for any follow-ups for the next 12 years, years. Our clinical case has been followed up after 12 years, with the
until 2 months before she was due to get married. reattached fragments still as good as they were initially.
The reattached fragments could have continued to perform well if
Dental Practice I March-April 2025 I Vol 21 No 2 39