
Page 18 - DP20-2.qxd
P. 18
implantology section
BOUND DOWN SOFT TISSUE AND THE
CRESTAL SOFT TISSUE COMPLEX IN
IMPLANT DENTISTRY- AN INSIGHT
Yazad Gandhi
When rehabilitating a patient with dental implants, we often notice
soft tissue deficiencies in quality and/or quantity. The development
of a sufficient peri-implant soft tissue cuff plays a significant role in
influencing the long-term stability of the surrounding bone and soft
tissues, as well as the seamless emergence of the superstructure into
the oral environment. This also contributes to establishing a condition
free of inflammation over the long term. Although numerous studies
over the years have proven that keratinized tissue around an implant
is essential to enhance the protective environment for the crestal bone,
Wennström et al suggested that further research is required to explore
the importance of keratinized tissue around implants and determine
the precise amount of soft tissue necessary to effectively prevent peri-
implant disease.
The controversy about the need for a keratinized (attached)
gingival zone around implant-supported restorations is a topic for
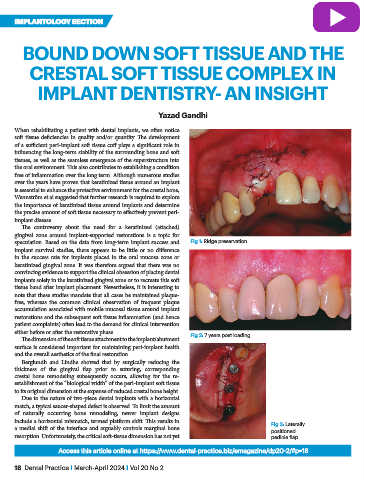
speculation. Based on the data from long-term implant success and Fig 1: Ridge preservation
implant survival studies, there appears to be little or no difference
in the success rate for implants placed in the oral mucosa zone or
keratinized gingival zone. It was therefore argued that there was no
convincing evidence to support the clinical obsession of placing dental
implants solely in the keratinized gingival zone or to recreate this soft
tissue band after implant placement. Nevertheless, it is interesting to
note that these studies mandate that all cases be maintained plaque-
free, whereas the common clinical observation of frequent plaque
accumulation associated with mobile mucosal tissue around implant
restorations and the subsequent soft tissue inflammation (and hence
patient complaints) often lead to the demand for clinical intervention
either before or after the restorative phase. Fig 2: 7 years post loading
The dimension of the soft tissue attachment to the implant/abutment
surface is considered important for maintaining peri-implant health
and the overall aesthetics of the final restoration.
Berglundh and Lindhe showed that by surgically reducing the
thickness of the gingival flap prior to suturing, corresponding
crestal bone remodeling subsequently occurs, allowing for the re-
establishment of the “biological width” of the peri-implant soft tissue
to its original dimension at the expense of reduced crestal bone height.
Due to the nature of two-piece dental implants with a horizontal
match, a typical saucer-shaped defect is observed. To limit the amount
of naturally occurring bone remodeling, newer implant designs
include a horizontal mismatch, termed platform shift. This results in Fig 3: Laterally
a medial shift of the interface and arguably controls marginal bone positioned
resorption. Unfortunately, the critical soft-tissue dimension has not yet pedicle flap
Access this article online at https://www.dental-practice.biz/emagazine/dp20-2/#p=18
18 Dental Practice I March-April 2024 I Vol 20 No 2