
Page 44 - DP20-2.qxd
P. 44
implantology section
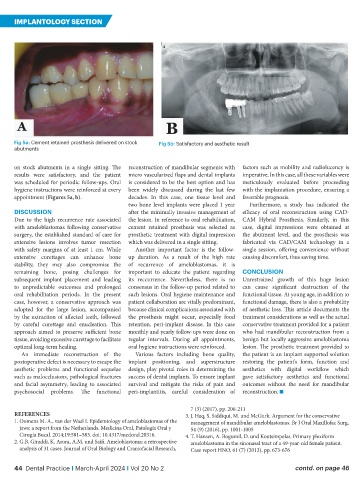
Fig 5a: Cement retained prosthesis delivered on stock Fig 5b: Satisfactory and aesthetic result
abutments
on stock abutments in a single sitting. The reconstruction of mandibular segments with factors such as mobility and radiolucency is
results were satisfactory, and the patient micro vascularized flaps and dental implants imperative. In this case, all these variables were
was scheduled for periodic follow-ups. Oral is considered to be the best option and has meticulously evaluated before proceeding
hygiene instructions were reinforced at every been widely discussed during the last few with the implantation procedure, ensuring a
appointment (Figures 5a, b). decades. In this case, one tissue level and favorable prognosis.
two bone level implants were placed 1 year Furthermore, a study has indicated the
DISCUSSION after the minimally invasive management of efficacy of oral reconstruction using CAD-
Due to the high recurrence rate associated the lesion. In reference to oral rehabilitation, CAM Hybrid Prosthesis. Similarly, in this
with ameloblastomas following conservative cement retained prosthesis was selected as case, digital impressions were obtained at
surgery, the established standard of care for prosthetic treatment with digital impression the abutment level, and the prosthesis was
extensive lesions involves tumor resection which was delivered in a single sitting. fabricated via CAD/CAM technology in a
with safety margins of at least 1 cm. While Another important factor is the follow- single session, offering convenience without
extensive curettages can enhance bone up duration. As a result of the high rate causing discomfort, thus saving time.
stability, they may also compromise the of recurrence of ameloblastomas, it is
remaining bone, posing challenges for important to educate the patient regarding CONCLUSION
subsequent implant placement and leading its reccurrence. Nevertheless, there is no Unrestrained growth of this huge lesion
to unpredictable outcomes and prolonged consensus in the follow-up period related to can cause significant destruction of the
oral rehabilitation periods. In the present such lesions. Oral hygiene maintenance and functional tissue. At young age, in addition to
case, however, a conservative approach was patient collaboration are vitally predominant, functional damage, there is also a probability
adopted for the large lesion, accompanied because clinical complications associated with of aesthetic loss. This article documents the
by the extraction of affected teeth, followed the prosthesis might occur, especially food treatment considerations as well as the actual
by careful curettage and enucleation. This retention, peri-implant disease. In this case conservative treatment provided for a patient
approach aimed to preserve sufficient bone monthly and yearly follow-ups were done on who had mandibular reconstruction from a
tissue, avoiding excessive curettage to facilitate regular intervals. During all appointments, benign but locally aggressive ameloblastoma
optimal long-term healing. oral hygiene instructions were reinforced. lesion. The prosthetic treatment provided to
An immediate reconstruction of the Various factors including bone quality, the patient is an implant supported solution
postoperative defect is necessary to escape the implant positioning, and superstructure restoring the patient’s form, function and
aesthetic problems and functional sequelae design, play pivotal roles in determining the aesthetics with digital workflow which
such as malocclusions, pathological fractures success of dental implants. To ensure implant gave satisfactory aesthetics and functional
and facial asymmetry, leading to associated survival and mitigate the risks of pain and outcomes without the need for mandibular
psychosocial problems. The functional peri-implantitis, careful consideration of reconstruction. n
7 (3) (2017), pp. 206-211
REFERENCES 3. J. Haq, S. Siddiqui, M. und McGurk. Argument for the conservative
1. Oomens M. A., van der Waal I. Epidemiology of ameloblastomas of the management of mandibular ameloblastomas. Br J Oral Maxillofac Surg,
jaws; a report from the Netherlands. Medicina Oral, Patología Oral y 54 (9) (2016), pp. 1001-1005
Cirugía Bucal. 2014;19:581–583. doi: 10.4317/medoral.20316. 4. T. Hansen, A. Bogumil, D. und Koutsimpelas. Primary plexiform
2. G.B. Giraddi, K. Arora, A.M. und Saifi. Ameloblastoma: a retrospective ameloblastoma in the sinonasal tract of a 49-year-old female patient.
analysis of 31 cases. Journal of Oral Biology and Craniofacial Research, Case report HNO, 61 (7) (2013), pp. 673-676
44 Dental Practice I March-April 2024 I Vol 20 No 2 contd. on page 46